가와사키 병과 가와사키 병에 관한 백문 백답, Kawasaki disease (Mucocutaneous lymph node syndrome/Kawasaki syndrome) and one hundred questions and answers on Kawasaki disease
가와사키 병의 개요
- 가와사키 병의 원인은 확실히 모른다.
- 비교적 흔한 급성 전신 열병 발진성 질환이다.
- 가와사키 병을 피부 점막 림프절 증후군(Mucocutaneous lymphnode syndrome) 또는 가와사키 증후군이라고도 한다.
- 2차 세계대전이 끝난 바로 후 일본사람 가와사키가 가와사키 병이란 병명을 처음으로 붙였다.
- 그 후 이 병은 일본·한국·미국 등 세계 각처에서 발생됐다.
- 이 병은 주로 5세 이하 영유아들에게 생긴다.
- 동맥염, 맥관염, 피부염, 점막염, 림프절염 등이 전신에 생길 수 있다.
가와사키 병의 원인
- 바이러스, 박테리아, 또는 카펫 마이트 등 병원체 감염으로 가와사키 병이 생기는지 않는다.
- 원인을 확실히 모른다.
- 항원 항체 이상반응으로 생긴다고 믿는다. 그러나 감염병의 일종이라고 추정하기도 한다.
- 아시아 소아청소년들에게 이 병이 더 잘 생길 수 있으나 서양 소아청소년들이나 흑인 영유아 청소년들을 가릴 것 없이 각 인종 소아청소년들에게 이 병이 생길 수 있다.
- 남아들이 여아들보다 이 병에 더 잘 걸리고 신생아들도 사춘기 아이들도 이 병에 걸릴 수 있다.
- 생후 18~24개월 유아들에게 더 잘 발생된다.
- 사시사철 어느 철에도 발생될 수 있으나 겨울철 봄철에 더 잘 발생된다.
- 가습기를 사용하면 가와사키 병에 더 잘 걸릴 수 있다는 최근 연구도 있다.
가와사키 병의 증상 징후

사진 8-2. 가와사키 병으로 인한 혀의 변화. 성홍열이 있을 때 생긴 혀의 변화와 비슷하다.
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP

사진 8-3. 카와사키 병이 있을 때 목에 있는 림프절이 붓는 것이 보통이다.
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
- 나이·중증도·병일·합병증의 유무 등에 따라 증상 징후가 다르다.
- 생후 6개월 이전 영아가 이 병에 걸리면 인두통, 림프절 비대, 열 등이 나타날 수 있다. 드물게는 아무 증상 징후가 나타나지 않다가 갑자기 사망할 수 있다.
- 가와사키 병의 전형적인 증상 징후는 다음과 같다.
-
- 고열이 갑자기 나고
- 결막염으로 눈이 빨갛게 충혈이 되고
- 인두가 붓고 빨갛고
- 혓바닥이 붉은 딸기 모양으로 도돌도돌해질 수 있다.
- 입술이 붓고 갈라질 수 있고,
- 홍역 꽃이나 성홍열 꽃과 비슷한 피부 발진이 나 있을 수 있고
- 다형 홍반과 비슷한 다양한 피부 발진이 전신의 피부에 날 수 있다.
- 피부 표면에 납작하게 깔린 피부 발진, 사포 모래알 같이 도돌도돌한 피부 발진도 날 수 있다.
- 손발의 피부가 붓고 붉고 팽팽해질 수 있고
- 손가락의 피부의 표피가 얇게 벗겨질 수 있다.
- 한쪽 턱 밑 부위나 양쪽의 턱 밑 부위, 그 외 신체 다른 부위 림프절이 크게 붓을 수 있다.
- 그 림프절을 만지면 아프고 부드러운 촉감이 있다.
- 팔꿈치·팔목·무릎·발목 등의 관절이 붓고 만지면 따뜻하고 아프고 붉을 수 있다.
- 이 병을 앓는 아이들 중 10~40%는 심근경색증, 5%에서 심근염, 20%에서 심낭염과 심내막염, 20%에서 부정맥 등의 심장병이 생길 수 있다. 그로 인해 사망할 수 있다.
- 적절한 치료를 받지 않은 가와사키 병의 20~25%에서 관상동맥 확장 또는 관상 동맥 동맥류가 생길 수 있다.
- 입맛이 없고
- 전신이 아파서 보채고
- 콧물이 나면서 기침도 하며
- 설사·구토·복통·근육염·폐렴, 관절염 및, 또는 관절통(35%)· 무균성 뇌염(25%)· 홍채모양염· 전 포도막염(80%)· 전신 경련· 뇌신경 마비 등이 있을 수 있다.
- 이 병으로 인하여 신체의 여러 계통의 여러 기관들에 염증이 생길 수 있고
- 그 염증에 따른 증상 징후가 나타날 수 있다.
- 이 병은 전신 모든 계통의 여러 기관들에 생길 수 있는 전신 질환이라고 할 수 있다.
- 경과에 따라 이 병을 4기로 나눈다.
-
- 발병한 지 1~11일 기간을 급성기,
- 발병한 지 11~21일의 기간을 아 급성기,
- 발병한 지 21~60일의 기간을 회복기,
- 발병 후 1년까지 기간을 만성기라고 한다.
- 앞서 설명한 여러 증상, 징후와 합병증이 저마다 다르게 나타나고 때로는 불과 몇 가지의 증상만 나타날 수 있고, 또 많은 종류의 증상, 징후와 합병증이 함께 나타날 수 있다.
- 가와사키 병의 여러 증상 징후들 중 몇 가지만 나타날 때는 이 병을 진단하는 데 어려움이 있을 수 있다.
- 드물지만 이 병이 발병된 지 수개월 내지 2~3년 후에 심장 관상동맥 맥관염이 생겨 그로 인해 사망할 수 있다.
가와사키 병의 진단
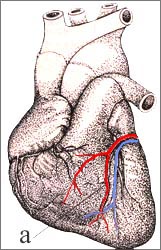
사진 8-4. 가와사키 병으로 심장병이 생길 수 있다.
a – 관상 동맥
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
- 병력·증상·징후·진찰소견 등을 종합해서 이 병을 진단할 수 있다.
- 미 CDC는 다음과 같은 증상, 징후, 조건이 있으면 가와사키 병을 진단할 수 있다고 했다.
- 섭씨 39도 이상 열이 5일 또는 그 이상 동안 나면서 적어도 다음 4가지 증상이나 징후가 있으면 가와사키 병을 진단할 수 있다고 한다.
① 양쪽 눈이 붉고 결막염이 있고
② 점막이 붉고 갈라지고, 인두가 발적되고, 붉은 딸기 모양의 혀가 있고
③ 국소적으로 또는 전신적으로 피부발진이 나고
④ 한쪽 또는 양쪽의 경부 림프절의 직경이 1.5cm이거나 그 이상 더 크게 붓고
⑤ 손바닥이나 발바닥에 홍반이 생기고 손이나 발이 붓고 전신적으로나 손톱 주위에 탈피가 생기는 증상 징후 중 적어도 한 가지 증상 징후가 있으면 가와사키 병을 진단할 수 있다.
- 다시 설명하면, 이상 증상 징후들 중 적어도 4가지 이상의 증상 징후와 열이 있으면 가와사키 병을 진단할 수 있다(출처: Pediatric News, July 2007).
- 대개 이 병이 발병된 후 처음 며칠 동안 이 병을 앓고 있는지 다른 병을 앓고 있는지 의사들도 엄마 아빠들도 확실히 몰라 확실한 진단 없이 지낼 수 있다.
- 확실한 진단이 나기까지 여러 의사들의 검진을 받고 여러 병원을 방문할 수 있다. 그러나 병이 점점 더 진행됨에 따라 진단이 확실히 나오게 된다.
- 급성기의 전형적인 가와사키 병은 앞서 설명한 여러 가지 증상 징후를 종합해서 비교적 쉽게 진단할 수 있다.
- CBC 피 검사, CRP, ESR, 대소변 세균검사, 가슴 X-선 검사, 심전도, 심장 에코검사 등의 결과를 참조해 이 병을 진단하는데 도움 얻는다.
-
- 알부민 혈중 농도가 3g/dl이거나 그 이하이고,
- 헤모글로빈(혈색소) 농도가 낮고,
- 발병 7일 후에 혈소판 수가 450,000/mdL이거나 그 이상,
- 백혈구수가 15,000/mcL거나 그 이상,
- 소변 백혈구수가 10/HPF이거나 그 이상이면
- 진단하는데 많은 도움이 된다.
- 가와사키 병이 있는 아이들의 79%에서 농뇨(Pyuria)가 생긴다. (출처;Infectious Disease in Children July 2009 p.19).
표 8-1. 가와사키 병 감별 진단
| 감별 진단 |
|
출처와 참조문헌; Manual of emergency pediatrics 4th edition, Robert M. Reece, M.D., p.450. [부모도 반의사가 되어야 한다-소아가정간호백과]-제 11권 소아 심장 혈관 질환-가와사키 심장염
가와사키 병의 치료
- 특효약은 아직 없다.
- 이 병으로 인한 여러 증상 징후에 따라 대증 치료를 한다.
- 1일 아스피린 총 치료 용량은 체중 매 kg당 100mg이다. 그 1일 총 치료 용량을 4 등분해서 통증, 열, 전신성 권태감 등의 증상 징후가 다 없어질 때 까지 약 8주~3개월 간 치료한다.
- 그 다음은 동맥류, 혈전, 혈소판 과다증을 예방하기 위해 1일 아스피린 체중 매 kg당 3~5mg을 매일 2개월간 복용하든지 심장 이상이 없을 때까지 복용한다.
- 이 병이 의심되거나 진단이 나면 감마 글로불린(IVIG) 체중 매 kg당 2g 정맥주사로 치료 한다. 특히 이 병으로 인해 열이 생기기 시작한 날로부터 10일 내에 감마 글로불린 정맥 주사로 치료하면 관상동맥류 발생률을 5%까지 경감시킬 수 있다.
- 감마 글로불린 정맥주사(IVIG)와 프레드니솔론(Prednisolone)의 치료 효과가 더 좋다고 한다(출처: Infectious Disease in Children July 2009 p.19).
- 심장 관상동맥염은 아스피린으로 오랫동안 치료한다.
- 앓고 있는 동안은 물론이고 회복이 다 된 이후에도 소아 심장전문의의 치료를 계속 받아야 한다.
■ 가와사키 병에 관한 백문 백답
Q.
가와사키 증후군(가와사키 병)의 원인은 무엇인가?
A.
감염병의 일종이라고 추정하지만 확실한 원인은 아직 모른다.
Q.
소아청소년들 중 특수 연령층에게 가와사키 증후군은 더 잘 발생되나?
A.
생후 6개월에서부터 사춘기까지 나이를 가리지 않고 생길 수 있다. 그러나 가와사키 병에 걸린 소아청소년들의 80%는 5세 이전 영유아들이다.
Q.
가와사키 병의 증상 징후는 일률적으로 나타나는가?
A.
증상 징후와 정도에 따라 전형적인 가와사키 병과 비전형적 가와사키 병으로 나눌 수 있다.
증상 징후와 정도가 일률적이 아니다.
Q.
비전형적 가와사키 병은 어떤 연령층의 아이들에게 더 잘 발생되나?
A.
비전형적인 가와사키 병은 1세 이전 영아들에게 더 잘 나타날 수 있다.
Q.
전형적 가와사키 병의 증상 징후는 어떤 것이 있나?
A.
양쪽 눈 결막염
구강 점막과 인두점막이 붉고 붉은 딸기양의 혀, 붉고 갈라진 입술
다양성 피부 발진
손바닥과 발바닥에 홍반성 발진과 손과 발이 붓고 손발 손톱 주위의 탈피
목의 림프절이 적어도 직경 1.5cm 이상 커 지고 그 림프절 속에 고름은 잡히지 않고
열이 적어도 5일 이상 나고(드물게는 열이 나지 않는다)
보채고 예민하고 복통, 설사, 구토, 요도염, 관절염, 뇌막염, 심막염, 심근염, 담낭염 등 증상 징후 합병증 중 일부나 전부를 동반할 수 있다.
Q.
비전형적인 가와사키 병의 증상 징후는 어떤 것이 있나?
A.
전형적인 가와사키 병의 증상 징후의 일부만 나타날 수 있다. 그 증상 징후의 정도에 차이가 있다.
Q.
가와사키 병의 발생이 계절에 따라 차이가 있는가?
A.
미국에서는 겨울과 가을철에 더 많이 발생된다.
Q.
가와사키 병을 특별히 진단하는 방법이 있는가?
A.
없다. 그러나 병력, 가족병력, 증상, 징후, 진찰소견, 임상검사, 병의 경과 등을 총 종합해 진단한다.
Q.
가와사키 병 치료에 특효약이 있나?
A.
특효약은 없지만 가와사키 병으로 인한 증상 징후 및 염증을 경감시키는 약이 있다.
Q.
가와사키 병 치료에 주로 쓰는 항 염증제는 무엇이 있는가?
.A.
아스피린, 감마 글로불린, 코르티코스테로이드제 등이 있다.
Q.
이 병의 치료에 아스피린을 쓰는 이유
A.
아스피린은 해열 진통 소염 작용이 있고 혈액 응고 기능을 감소시키는 약리작용이 있다.
Q.
아스피린으로 치료할 때 아스피린의 용량은
A.
급성기 가와사키 병을 치료 하는 데는 아스피린 체중 매 kg당 80~100mg을 1일 총 용량으로 계산해서 그 1일 총 용량을 4 등분해서 4회 경구 복용한다. 그리고 열이 떨어지고 증상 징후가 아주 호전 된 4~5일 이후부터 아스피린 체중 매 kg당 3~5mg을 1일 1회 복용한다.
Q.
아스피린 치료는 언제부터 시작하나?
A.
이 병을 의심하거나 진단을 받으면 바로 아스피린 치료를 시작한다.
이 병이 발병된 6~8주 이후까지 심장 관상동맥에 아무 이상이 없으면 아스피린 치료를 중지하는 것이 보통이다.
관상동맥에 이상이 있을 때는 아스피린 치료를 계속 받아야 한다.
Q.
아스피린으로 치료 받을 때 어떤 부작용이 생길 수 있나?
A..
아스피린 약물 알레르기, 출혈, 소화장애, 라이 증후군 등이 드물게 생길 수 있다.
Q.
감마 글로불린 치료는 언제부터 시작하나요?
A.
가와사키 병을 앓는다고 의심하거나 진단을 받은 후 가능하면 곧 치료를 시작하는 것을 권장한다.
가와사키 병을 의심하면 감마 글로불린 치료를 바로 시작한다. 이렇게 조기치료를 했다고 해서 과다 치료를 했다고 걱정할 것 없다고 한다(Pediatric News, July 2007).
일반적으로 아스피린으로 치료 받을 때보다 감마 글로불린과 아스피린으로 동시 치료받으면 심장 관상동맥 이상이 덜 생기고 열이 쉽게 떨어지고 염증이 더 빨리 회복된다고 한다. 그런 이유로 진단을 받은 후 곧 시작한다. 적어도 발병 후 10일 이전부터 시작하는 것이 좋다.
Q.
감마 글로불린으로 치료하면 심장 관상동맥 이상이 생기지 않는가?
A.
생기는 확률이 아주 줄어든다.
Q.
감마 글로불린의 치료용량은 얼마인가?
A.
가장 적절한 감마 글로불린의 치료 용량에 관해 확실히 모르나 체중 매 kg당 2g을 1회 용량을 정맥주사로 치료한다.
Q.
감마 글로불린과 아스피린으로 치료하면 모든 환자가 완치되나?
A.
드물게는 열과 다른 증상 징후가 계속되거나 재발할 수 있다.
Q.
이 병으로 인해 심장에 어떤 이상이 생겨 있는지 어떻게 알아보나?
A.
가와사키 병이 있다고 의심하거나 진단을 받았을 때 심장 에코검사를 받고 이 병이 시작한 날로부터 6~8주에 또다시 검사받는 것이 일반적이다. 그러나 이 병의 경과에 따라 이런 검사를 더 자주 받을 수 있다.
Q.
이 병을 앓으면 소아 심장내과 전문의의 치료를 받아야 하는 이유
A.
위에서 설명한바와 같이 이 병을 앓는 아이들의 일부에게 심장 관상동맥염, 심근염, 심막염이 생길 수 있다. 소아 심장내과 전문의의 도움으로 진단 치료를 받는 것이 중요하다.
또 이 병으로 심장에 어떤 이상이 있나 적절한 간격을 두고 추적 검진 진단을 받고 적절히 치료 받는 것이 중요하고 심장 이상이 있을 때는 필요에 따라 아스피린으로 치료받습니다.
|
다음은 “가와사키 병”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q.&A. 가와사키 병
Q.
안녕하십니까?
본 홈페이지를 운영하면서 불특정다수에게 많은 관심과 사랑으로 의료에 대해 쉽고 명쾌하게 답변해 주신다는 점을 듣고….송구스럽게도 찾아뵈어야 하지만 지면으로나마 몇 글자 올립니다.. 다름이 아니라 제목에서 언급한 것처럼 울 큰아이가(만4세) 병원진단결과 가와사끼병에 걸렸다는군요… 순간 너무 당혹한 나머지 정신마저 몽롱해질 뻔 했습니다…
무지에서 오는 당혹감도 있었지만 질병과 관계되는 사이트를 찾으면 찾을수록 더욱더 신경이 예민해지는군요
엄청난 기술(의료기술도 포함하여)의 발달로 웬만한 질병이외엔 모두 치료가능하고 완쾌될 수 있다는 의료인에 대한 믿음으로 지금도 살고 있지만 정보검색결과 원인이 무엇인지 아직도 명확한 규정이 없더군요…ㅠ.ㅠ 원인이 무엇인지 ….왜 그러한 질병이 닥치는지를 알아야 그에 대한 대책과 모색을 할 것인데…..
선생님….감히 부탁드립니다…. 치료과정 및 치료 후에 저희 엄마아빠가 어떠한 사항에 대하여 어떻게 대처해 나가야 하는지 ……또한 생활과정에서 아이에게 부적절한 행동양식이나 부적절한 식사법 등 …….참으로 알고 싶은 것이 많습니다….
한 아이의 엄마아빠로서 치료전반에 걸쳐 기간별로 명쾌한 설명을 부탁드리며….또한 엄마아빠의 대처방법을 가르쳐 주었으면 합니다…..
RE-의 답변 꼬옥 기다리겠습니다…. <참고> 현재 급생식기에 면역글로블린의 약제를 투여 후 여러 증상들이 호전되고 있는 중입니다…..정보 사이트를 기준으로 하면 현재는 아급 생식기에 해당되는 것으로 사료됩니다….
A.
안녕하세요. 좋은 질문을 해주시고 저를 칭찬을 많이 해 주셔서 대단히 감사합니다. 저의 홈페이지에서 많은 소아청소년 건강과 양육에 도움이 된다는 말씀을 들을 때 저는 즐겁습니다. 감사합니다.
자녀의 나이, 성별, 과거의 병력, 가족의 병력, 진찰소견, 임상검사 등 정보를 많이 알수록 더 좋은 답변을 들일 수 있습니다. 주신 정보를 토대로 해서 답변을 드립니다.
가와사키 병의 원인은 아직도 확실히 모릅니다. 바이러스 감염으로 생기나 의심해 보았지만 증명해내지 못했습니다.
제 자신도 가와사키 병을 앓는 환아들을 여러 명 진료했지만 합병증과 후유증 없이 완치됐습니다. 너무 걱정 마시고 잘 낫도록 많이 기도하시기 바랍니다.
물론 엄마아빠가 걱정하시는 것을 다 이해할 수는 없을 겁니다.
이 병이 있으면 일반적으로 종합병원 소아청소년과 전문의, 소아 심장 전문의, 류마티스 병 전문의 등으로 이루어진 치료 팀 멤버가 서로 자문하면서 함께 치료하는 것이 일반적입니다. 아시겠지만 저는 소아청소년과 전문의입니다.
감마글로불린 혈관주사로 발병 후 첫 10일 내 치료하면 열나는 기간이 단축될 수 있고 관상동맥 확장증과 관상동맥류의 발생률이 3% 이하로 감소될 수 있다고 합니다.
감마글로불린 혈관주사 치료 이외 아스피린으로 염증과 혈소판 장애를 치료하는 것이 보통입니다.
아스피린으로 열이 떨어질 때까지 치료하고 적혈구침강속도(ESR) 검사의 결과와 혈소판 수치가 정상으로 돌아갈 때까지 또는 발병 후 6~8주 동안 적극적으로 치료하는 것이 보통입니다.
어떤 의사들은 관상동맥 이상이 있을 때는 더 오랫동안 아스피린으로 치료하라고 합니다.
심장 X-선 사진, 심전도 검사와 심장 초음파 검사로 심장 이상이 있는지 알아보고 그 후 6~8주에, 또 6~12개월에 그런 검사를 반복하는 것이 보통입니다. 물론 증상 징후에 따라서 더 자주 더 오랫동안 그런 검사를 하고 진찰, 진단 치료를 받아야 합니다. 보통 소아 심장 전문의로부터 추적치료를 받는 것이 좋습니다.
관상동맥에 아무 이상이 없는 환아는 진단받은 후 6~8주부터는 육체적 활동을 제한하지 않습니다.
일시적으로 관상동맥 이상이 있을 때는 진단 받은 6~8주 이후부터는 육체적 활동을 제한하지 않습니다.
관상동맥류가 작은 관성동맥에 생겼거나 중등도 관성동맥에 생겼거나 그 수가 하나만 있을 때는 관상동맥류를 진단한 후 6~8주 이후부터 육체적 활동을 제한하지 않습니다.
10세 이전 환아의 관상동맥에 생긴 동맥류가 작든지 크든지 동맥이 막히지 않았을 때도 6~8주 이후부터 육체적 활동을 제한하지 않습니다.
관상동맥이 막혔을 때는 접촉성 육체 운동 및 다른 몇 가지 육체적 운동을 제한합니다.
이상 설명한 치료 등을 존 홉킨스 의과대학에서 발간한 참고서에서 얻은 정보의 일부입니다.
이러한 복잡한 육체적 활동의 제한이나 제한할 육체적 운동의 종류나 기간이나 치료 등은 어디까지나 각 환아의 병세의 중증도와 주치의의 판단에 따라 그때그때 적절히 조절하면서 치료하는 것이 원칙입니다.
일반적으로 섭취하는 음식물의 종류와 양에는 제한하지 않으나 여기에도 그때그때의 증상 징후와 합병증의 유무에 따라 적절히 조절해야 합니다.
가와사키 병에 대해서 더 자세히 말씀을 드리려면 더 많은 시간이 필요합니다.
가와사키 병은 일본이나 한국 등에서 더 잘 발생되고 그에 대한 치료에 관해서 그곳 의료진이 더 잘 아시는 줄로 알고 있습니다.
가와사키 병의 아급성기는 보통 발병 후 11~25일 기간을 의미합니다.
이 때 열, 발진, 림프절 비대 등이 없어지고 손가락이나 발가락의 피부에 표피탈락이 생기고 혈소판 수치가 증가됩니다.
치료를 받지 않은 전형적인 가와사키 병을 앓는 환아들의 15~25%에게 심장의 관상동맥염과 관상동맥류가 생길 수 있습니다. 일반적으로 발병 후 2~4주에 가장 많이 생기고 드물게는 6주 후에도 생깁니다.
그 외에 심장염, 대동맥판 역류, 승모판 역류, 삼천판 역류 등이 생길 수 있습니다.
심막염, 심우혈증, 좌심실 부전증 등이 생길 수 있습니다.
궁금증이 있으시면 단골 소아청소년에 문의하시기를 바랍니다.가와사키 병을 참조하시기 바랍니다. 질문이 더 있으시면 다시 연락 주시기 바랍니다. 감사합니다.
이상원 드림
|
다음은 “가와사키 병인지?”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q.&A. 가와사키 병인지?
Q.
현재 만30개월 남아입니다.
6월경에 수족구인 줄 알고 지나갔는데, 지금에 와서야 생각해보니 가와사카였을 가능성도 있었던 것 같아서 문의 드립니다. 손발바닥발진이 거의 4 주간 있었구요, 며칠간은 손이 퉁퉁 부었었습니다. 고열은 오래 가지 않았고(2~3일정도) 입안의 발진도 며칠 있었구요.
가와사키 병도 그냥 가볍게 지나갈 수 있는지요? 지금이라도 심장검사를 해볼 필요성이 있는 건지요? 혹시 나중에라도 후유증으로 남을 수가 있는 건지요?
A.
문호님
안녕하세요. 질문해 주셔 감사합니다.
아이의 나이, 성별, 과거와 가족의 병력, 진찰소견, 임상검사 결과 등 많은 정보가 있으면 더 좋은 답변을 드릴 수 있습니다. 주신 정보를 참작해 답변을 드립니다.
가와사키 병을 앓을 때 생기는 증상 징후가 전형적으로 나타날 수도 있고 때로는 비전형적으로 나타날 수 있습니다.
따라서 아기가 가와사키 병을 앓았을 가능성을 배제할 수 없습니다.
그래서 심장에 어떤 이상이 있는지 적어도 한번정도 알아보는 것도 좋을 것 같습니다.
소아청소년과에서 진찰 진단을 받으시고 그 문제에 관해 상담하시기 바랍니다.
성홍열, 수족구병, 가와사키 병. [부모도 반의사가 되어야 한다–소아가정간호백과]-제 15권 소아청소년 알레르기 및 자가면역 질환–연소성 류마토이드 관절염 등을 참조하시기 바랍니다. 질문이 더 있으면 또 방문하세요. 감사합니다. 이상원 드림
Kawasaki disease (Mucocutaneous lymph node syndrome/Kawasaki syndrome) and one hundred questions and answers on Kawasaki disease
Overview of Kawasaki Disease
• The cause of Kawasaki disease is unknown.
• Relatively common acute systemic fever rash.
• Kawasaki disease is also called mucocutaneous lymphnode syndrome or Kawasaki syndrome.
• Shortly after the end of World War II, Kawasaki was the first to name the disease Kawasaki disease.
• Since then, the disease has spread all over the world, including Japan, Korea, and the United States.
• This disease mainly affects children under 5 years of age.
• Arteritis, vasculitis, dermatitis, mucositis, and lymphadenitis can occur throughout the body.
Causes of Kawasaki disease
• Kawasaki disease is not caused by infection with pathogens such as viruses, bacteria, or carpet mite.
• The cause is not known for sure.
• Believed to be caused by an antigen-antibody adverse reaction. However, it is also presumed to be a type of infectious disease.
• Asian children and adolescents are more likely to develop the disease, but it can affect children of all races, whether it is western children or black infants and young people.
• Boys are more prone to the disease than girls, and newborns and adolescents can get it.
• It is more common in infants 18 to 24 months of age.
• It can occur at any time of the year, but it is more common in winter and spring.
• Recent studies suggest that using a humidifier may make you more susceptible to Kawasaki disease.
Symptoms of Kawasaki disease
Picture 8-2. Changes in the tongue due to Kawasaki disease. It is similar to the change in the tongue that occurs during scarlet fever. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
Picture 8-3. Swelling of the lymph nodes in the neck is common with Kawasaki disease. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
• Symptoms vary depending on age, severity, date of illness, and presence or absence of complications.
• If infants before 6 months of age develop this disease, sore throat, enlarged lymph nodes, and fever may occur. Rarely, there may be no symptoms and sudden death.
• Typical symptoms of Kawasaki disease are:
• o Sudden high fever
o Conjunctivitis causes red and bloodshot eyes
o The pharynx is swollen and red
o The tongue may be bulging in the shape of a red strawberry.
o Lips may become swollen and cracked,
o You may have a skin rash that resembles a measles flower or scarlet fever flower.
o Various skin rashes similar to erythema multiforme may appear on the skin all over the body.
o A skin rash that is spread flat on the skin surface or a skin rash that is rough like sandpaper grains may also occur.
o The skin on the hands and feet may become swollen, red, and tight
o The epidermis of the skin of the fingers may peel off thinly.
o Lymph nodes in one or both sides of the chin or in other parts of the body may swell significantly.
o The lymph nodes are painful and soft to the touch. o Joints such as elbows, wrists, knees, and ankles are swollen and may be warm, painful, and red to the touch.
o Among children with this disease, 10% to 40% of children may develop heart disease such as myocardial infarction, myocarditis in 5%, pericarditis and endocarditis in 20%, and arrhythmia in 20%. This could result in death.
o Coronary artery dilatation or coronary artery aneurysm can occur in 20-25% of Kawasaki’s disease without adequate treatment.
o I have no appetite o I feel sick all over my body o Have a runny nose and cough
o Diarrhea, vomiting, abdominal pain, myositis, pneumonia, arthritis and/or arthralgia (35%), aseptic encephalitis (25%), iritis, anterior uveitis (80%), generalized convulsions, cranial nerve palsy, etc.
o This disease can cause inflammation in various organs in various systems of the body.
o Symptoms may appear according to the inflammation.
o This disease can be said to be a systemic disease that can occur in various organs of all systems.
• Divide the disease into 4 stages according to the course.
• o 1 to 11 days after onset of acute phase,
o The period from 11 to 21 days after onset is subacute,
o 21 to 60 days after the onset of the recovery period;
o The period from onset to 1 year is called the chronic phase.
• Many of the symptoms, signs and complications described above appear differently, and sometimes only a few symptoms may appear, and many types of symptoms, signs and complications may appear together.
• Diagnosis of Kawasaki disease can be difficult when only a few of the symptoms are present.
• In rare cases, cardiac coronary vasculitis can develop and cause death several months to two to three years after the onset of the disease.
Diagnosis of Kawasaki disease
Picture 8-4. Kawasaki disease can lead to heart disease. a – coronary artery
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
• This disease can be diagnosed by combining medical history, symptoms, signs, and examination findings.
• According to the US CDC, Kawasaki disease can be diagnosed if the following symptoms, signs, and conditions are present.
• Kawasaki disease can be diagnosed if you have a fever of 39 degrees Celsius or higher for 5 days or longer and have at least the following 4 symptoms or signs.
① Both eyes are red and have conjunctivitis
② The mucous membrane is red and cracked, the pharynx is red, and there is a red strawberry-shaped tongue.
③ Local or systemic skin rash
④ One or both cervical lymph nodes with a diameter of 1.5 cm or larger swelling ⑤ Kawasaki disease can be diagnosed if there is at least one symptom of erythema on the palms or soles of the feet, swelling of the hands or feet, and molting systemically or around the nails.
• In other words, Kawasaki disease can be diagnosed if there are at least four or more symptomatic signs and fever (Source: Pediatric News, July 2007).
• Usually in the first few days after the onset of the disease, doctors and moms and dads are not sure whether they are suffering from this disease or another disease, so they can go without a definitive diagnosis.
• You can have multiple doctors’ checkups and visit multiple hospitals until a definitive diagnosis is made. However, as the disease progresses, the diagnosis becomes clear.
• Typical acute Kawasaki disease can be diagnosed relatively easily by combining the various symptoms described above.
• Get help in diagnosing this disease by referring to the results of CBC blood test, CRP, ESR, stool and urine bacteriology, chest X-ray, electrocardiogram, and echocardiography.
• o an albumin blood level of 3 g/dl or less; o Low hemoglobin (hemoglobin) concentration,
o Platelet count of 450,000/ml or higher 7 days after onset;
o WBC count of 15,000/mcL or higher;
o Urine WBC count of 10/HPF or higher
o It is very helpful in diagnosis.
o Pyuria develops in 79% of children with Kawasaki disease. (Source: Infectious Disease in Children July 2009 p.19).
Table 8-1. Differential diagnosis of Kawasaki disease differential diagnosis
| Differential diagnosis |
• measles, • Meningococcal bacteremia and sepsis; • scarlet fever; • Staphylococcal lacerated skin syndrome; • Rocky Mountain Erythema Fever; • anaphylactoid purpura; • Serum disease, etc. source |
sources and references; Manual of emergency pediatrics 4th edition, Robert M. Reece, M.D.,
www.drleepediatrics.com- Vol. 11 Children’s Cardiovascular Disease – Kawasaki Carditis Treatment of Kawasaki disease
• There is no specific drug yet.
• Treat symptomatically according to the various symptoms and signs of this disease.
• The total therapeutic dose of aspirin per day is 100 mg/kg body weight. The daily total therapeutic dose is divided into 4 equal parts and treated for about 8 weeks to 3 months until all symptoms such as pain, fever, and general malaise disappear.
• Next, to prevent aneurysm, thrombosis, and thrombocytopenia, take 3 to 5 mg of aspirin per kg of body weight daily for 2 months or until there are no heart problems.
• If this disease is suspected or diagnosed, gamma globulin (IVIG) is administered intravenously at 2 g/kg of body weight. In particular, intravenous gamma globulin treatment within 10 days of the onset of fever due to this disease can reduce the incidence of coronary aneurysm by 5%.
• Intravenous gamma globulin (IVIG) and Prednisolone have been shown to be more effective (Source: Infectious Disease in Children July 2009 p.19).
• Heart coronary arteritis is treated with aspirin for a long time. • Continue to see a pediatric cardiologist during illness and after recovery is complete.
■ 100 Questions and Answers on Kawasaki Disease Q. What causes Kawasaki syndrome (Kawasaki disease)?
A. It is believed to be some kind of infectious disease, but the exact cause is still unknown. Q. Is Kawasaki Syndrome more likely to occur in special age groups among children and adolescents?
A. It can occur at any age, from 6 months of age to puberty. However, 80% of children and adolescents with Kawasaki disease are children before the age of five.
Q. Do the symptoms of Kawasaki disease appear uniformly?
A. According to symptom signs and severity, Kawasaki disease can be divided into classic Kawasaki disease and atypical Kawasaki disease. Symptoms Signs and severity are not uniform.
Q. In what age group is atypical Kawasaki disease more likely to occur?
A. Atypical Kawasaki disease is more likely to appear in infants before the age of 1 year.
Q. What are the symptoms of classic Kawasaki disease?
A. bilateral eye conjunctivitis The oral mucosa and pharyngeal mucosa are red and red, the tongue of a strawberry sheep, and red and cracked lips Variety Skin Rash An erythematous rash on the palms and soles of the feet, swelling of the hands and feet, and peeling around the nails of the hands and feet The lymph node in the neck grows at least 1.5 cm in diameter, and pus is not trapped in the lymph node. Have a fever for at least 5 days (rarely any fever) It is irritating and sensitive and may accompany some or all of the symptomatic and symptomatic complications such as abdominal pain, diarrhea, vomiting, urethritis, arthritis, meningitis, pericarditis, myocarditis, and cholecystitis.
Q. What are the symptoms of atypical Kawasaki disease?
A. Only a subset of the symptoms of typical Kawasaki disease may appear. There is a difference in the severity of the symptoms.
Q. Does the incidence of Kawasaki disease vary by season?
A. In the United States, it is more common in winter and autumn.
Q. Is there a special way to diagnose Kawasaki disease?
A. does not exist. However, the diagnosis is made by synthesizing the medical history, family history, symptoms, signs, examination findings, clinical examination, and the course of the disease.
Q. Is there a specific drug for the treatment of Kawasaki disease?
. There is no specific drug, but there are drugs that relieve symptoms and inflammation caused by Kawasaki disease.
Q. What are the main anti-inflammatory drugs used to treat Kawasaki disease.
A. These include aspirin, gamma globulin, and corticosteroids.
Q. Why is aspirin used to treat this disease?
A. Aspirin has antipyretic, analgesic, and an
ti-inflammatory properties and has pharmacological actions that reduce blood clotting.
Q. When treated with aspirin, the dose of aspirin is
A. For the treatment of acute Kawasaki disease, 80-100 mg of aspirin per kg of body weight is calculated as the total daily dose, and the total daily dose is divided into 4 equal portions and taken orally 4 times. After 4-5 days after the fever has dropped and symptoms have improved significantly, aspirin 3 to 5 mg per kg of body weight is taken once a day.
Q. When does aspirin treatment start?
A. If the disease is suspected or diagnosed, start aspirin treatment immediately. Aspirin treatment is usually discontinued if there is no abnormality in the coronary arteries until 6-8 weeks after the onset of the disease. Aspirin treatment should be continued if coronary artery disease is present.
Q. What are the possible side effects of being treated with aspirin?
A.. Aspirin drug allergy, bleeding, digestive disorders, and Reye’s syndrome may occur infrequently.
Q. When does gamma globulin therapy start?
A. It is recommended to start treatment as soon as possible after being suspected or diagnosed with Kawasaki disease. If Kawasaki disease is suspected, gamma globulin therapy is started immediately. It is said that there is no need to worry about overtreatment because of this early treatment (Pediatric News, July 2007). In general, co-treatment with gamma globulin and aspirin results in fewer coronary artery anomalies lower fever, and faster inflammation recovery than when treated with aspirin. For that reason, it is started soon after being diagnosed. It is recommended to start at least 10 days before the onset of the disease.
Q. Does treatment with gamma globulin not cause cardiac or coronary anomalies?
A. The probability of occurrence is greatly reduced.
Q. What is the therapeutic dose of gamma globulin?
A. Although it is unclear about the most appropriate therapeutic dose of gamma globulin, a single dose of 2 g/kg of body weight is administered intravenously.
Q. Can all patients be cured by treatment with gamma globulin and aspirin?
A. Rarely, fever and other symptomatic signs may persist or recur.
Q. How do I know what’s wrong with my heart because of this disease?
A. When a person suspects or is diagnosed with Kawasaki disease, it is common to have an echocardiogram of the heart, followed by another test 6 to 8 weeks after the onset of the disease. However, as the disease progresses, these tests may become more frequent. Q. Why you should see a pediatric cardiologist if you have this disease
A. As described above, some children with this condition may develop coronary artery disease, myocarditis, and pericarditis. It is important to get diagnostic treatment with the help of a pediatric cardiologist.
In addition, it is important to receive a follow-up checkup diagnosis at an appropriate interval to see if there is any abnormality in the heart due to this disease and to receive appropriate treatment.
The following is an example of a Q&A for health counseling for children and adolescents on the Internet regarding “Kawasaki disease”.
Q&A. Kawasaki disease
Q. Hello? While operating this website, I heard that they give easy and clear answers about medical care to unspecified people with a lot of interest and love. As if my eldest child (4 years old) was diagnosed with Kawasaki disease…
There was some embarrassment from ignorance, but the more I search for sites related to diseases, the more sensitive I get. I am still living with the belief in medical professionals that all diseases can be cured and cured with the development of tremendous technology (including medical technology), but as a result of information search, there is still no clear regulation on the cause… ㅠ.ㅠ We need to know what the cause is….why such a disease occurs, so that we can take countermeasures and search for it… Teacher….
Dare you please…. What should my mother and father deal with during the treatment process and after treatment… Also, in the course of life, inappropriate behavioral patterns or inappropriate eating methods for children, etc. . …there are many things I really want to know…
As a mother and father of one child, I would like a clear explanation for each period throughout the treatment… Waiting for RE-‘s reply…. <Reference> Currently, after administering immunoglobulin drugs to the rapid genital organs, various symptoms are improving. It is presumed to be….
A. Hello. Thank you very much for asking good questions and complimenting me a lot. I am happy to hear from my website that it is helpful for the health and nurture of many children and adolescents. thank you.
The more information you know, such as the child’s age, gender, past medical history, family history, examination findings, and clinical tests, the better the answer can be given. We will respond based on the information you have provided. The cause of Kawasaki disease is still unknown.
I suspected it was caused by a virus infection, but I couldn’t prove it. I myself have treated several children with Kawasaki disease, but they were cured without complications or after-effects. Please don’t worry too much and pray a lot for well.
Of course, you won’t be able to understand everything Mom and Dad are worried about. When this disease is present, it is common for members of a treatment team consisting of general hospital pediatric specialists, pediatric cardiologists, and rheumatologists to consult each other and treat together.
As you may know, I am a pediatrician. Treatment with intravenous gamma globulin injection within the first 10 days of onset may shorten the duration of fever and reduce the incidence of coronary atherosclerosis and coronary aneurysm to less than 3%. In addition to gamma globulin injections, aspirin is usually used to treat inflammation and platelet disorders.
Treatment is usually with aspirin until the fever subsides and aggressive treatment until ESR results and platelet counts return to normal, or 6 to 8 weeks after onset. Some doctors recommend that you take aspirin for a longer period of time if you have coronary artery problems. Cardiac X-rays, electrocardiography, and echocardiography are usually done to detect heart abnormalities and repeat these tests at 6 to 8 weeks and then at 6 to 12 months.
Of course, depending on the symptoms, you need to have such tests more often and for a longer period of time, and you should be diagnosed and treated. It is usually recommended to follow up with a pediatric cardiologist. Children with no abnormalities in the coronary arteries do not limit their physical activity from 6 to 8 weeks after diagnosis. If there is a temporary coronary artery abnormality, physical activity is not restricted from 6 to 8 weeks after diagnosis. If the coronary aneurysm develops in a small coronary artery, in a moderate coronary artery, or if there is only one, physical activity is not restricted from 6 to 8 weeks after the diagnosis of the coronary aneurysm.
Even if the aneurysm in the coronary artery of a child before the age of 10 years is small or large, and the artery is not blocked, physical activity is not restricted after 6-8 weeks. When a coronary artery is blocked, contact physical activity and some other physical activity are limited. The treatment described above is part of the information obtained from the reference book published by John Hopkins Medical School. In principle, the restriction of these complex physical activities or the type, period, or treatment of physical exercise to be restricted should be appropriately controlled and treated according to the severity of each patient’s condition and the judgment of the attending physician. In general, there are no restrictions on the type and amount of food consumed, but it should be appropriately adjusted according to the symptoms and complications at the time. We need more time to tell you more about Kawasaki disease.
I know that Kawasaki disease is more common in Japan and Korea, and the medical staff there knows better about treatment. The subacute phase of Kawasaki disease usually refers to a period of 11 to 25 days after onset. At this time, fever, rash, enlarged lymph nodes, etc. disappear, and the skin of the fingers and toes becomes exfoliated and the platelet count increases. Untreated, 15 to 25% of children with typical Kawasaki disease may develop coronary arteritis and coronary aneurysms of the heart. It usually occurs most often 2-4 weeks after onset, and rarely occurs even after 6 weeks. Carditis, aortic regurgitation, mitral regurgitation, and tricuspid regurgitation may also occur. Pericarditis, cardiomyopathy, and left ventricular insufficiency may occur. If you have any questions, please contact your regular pediatrician. Please refer to Kawasaki disease. If you have any more questions, please feel free to contact us again. thank you. Lee Sang-won .
The following is an example of a Q&A for health counseling for children and adolescents on the Internet about “Is it Kawasaki disease?”
Q&A. Is it Kawasaki disease?
Q. He is currently only 30 months old. I passed by thinking it was a hand, foot and mouth around June, but now that I think about it, it seems that it may have been Kawasaka, so I’m asking. I had plantar rash for almost 4 weeks, and my hands were swollen for a few days. The high fever did not last long (about 2-3 days) and there were also a few rashes in the mouth. Can Kawasaki disease just pass easily? Is it necessary to do a heart test right now? Could it be left behind as a sequelae in the future?
A. Moon Ho Hello. Thank you for asking a question. We can give you a better answer if you have a lot of information such as the child’s age, sex, past and family history, examination findings, and clinical test results. We will respond based on the information you have provided. The symptoms of Kawasaki disease can be typical or sometimes atypical. Therefore, the possibility that the baby has Kawasaki disease cannot be ruled out. So, it would be good to check at least once for any abnormalities in the heart. Please visit the Department of Pediatrics for diagnosis and consultation about the problem. Scarlet fever, hand, foot and mouth disease, Kawasaki disease. [Parents should also become at lerast the half-doctors-Children and Family Nursing Encyclopedia]-Volume 15 Children and Adolescents Allergy and Autoimmune Diseases-Children’s Rheumatoid Arthritis, etc. Please visit again if you have more questions. thank you. Lee Sang-won.
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989.
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
- Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
- Preparation for Birth. Beverly Savage and Dianna Smith
- Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- Clinical Atlas of Blood Diseases, Sixth Edition, A. Piney, M.D., and Stanley Wyard M.D., The Blakiston Co
- Hematologic Problems in The Newborn, Third Edition, Volume IV in the series, Major Problems in Clinical Pediatrics, Oski and Naiman, W.B. Saunders.
- Pediatric Hematology, The Pediatric Clinics of North America, June 1996, W.B. Saunders
- Pediatric Hematology, The Pediatric Clinics of North America, May 1980, W.B. Saunders
- 소아과학 대한교과서
- 의학 용어사전 대한 의사 협회
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.